The parameters of the ClinicalQ are intentionally not proprietary, freely published for any Clinician to apply in their assessments / treatments & training. They can be found in his book Adding Neurotherapy to Your Practice. https://www.soundhealthproducts.com/collections/books
We do however ask that the data & formulas are not commercialized (packaged within systems and equipment sold or otherwise used for profit). We remain saddened that this request has not been observed.
In the classification of wellness, non-clinical software and systems, Divergence has limited permission to use intellectual property of the ClinicalQ* (c.2015) in their TheraQ.*
Please note that the ONLY two Swingle vetted (checked for reliability and validity AKA accuracy), current (adapted & upgraded) and approved (obtained our permission to produce) program / assessment systems available for purchase* are produced by BFE (Biofeedback Federation of Europe) and now IFEN (Germany). The BFE Swingle ClinicalQ Software Suite runs on medical grade FDA and Health Canada Approved (Canadian equivalent of FDA) Thought Technology (Canada) equipment and is available for purchase through the Biofeedback Federation of Europe (BFE) website BFE. https://www.bfe.org/buy/1-dr-swingles-clinicalq-braindriver-suite-p-99.html The IFEN software runs on medical grade FDA approved BrainMaster compatible equipment.

The BFE (Biofeedback Federation of Europe) also sponsors Grand Rounds, wherein Dr Mari Swingle teaches and mentors use of the method.
IFEN (Institute for EEGNeeurofeedback, Germany) also offers Quarterly Grand Rounds with Dr Mari Swingle.
* Please contact the Swingle Clinic if you wish for permission(s) to commercialize or otherwise package our intellectual property including the formulas / parameters of the Swingle ClinicalQ in equipment and programs. We are open to collaborations.
*Swingle Holdings and subsidiaries thereof, including but not limited to owner, employees, contractors or representees assume no responsibility or liability, clinical or otherwise, for any application, use, or misuse of the ClinicalQ c.2015 or TheraQ.
Less time and money on assessment means more on treatment and betterment.
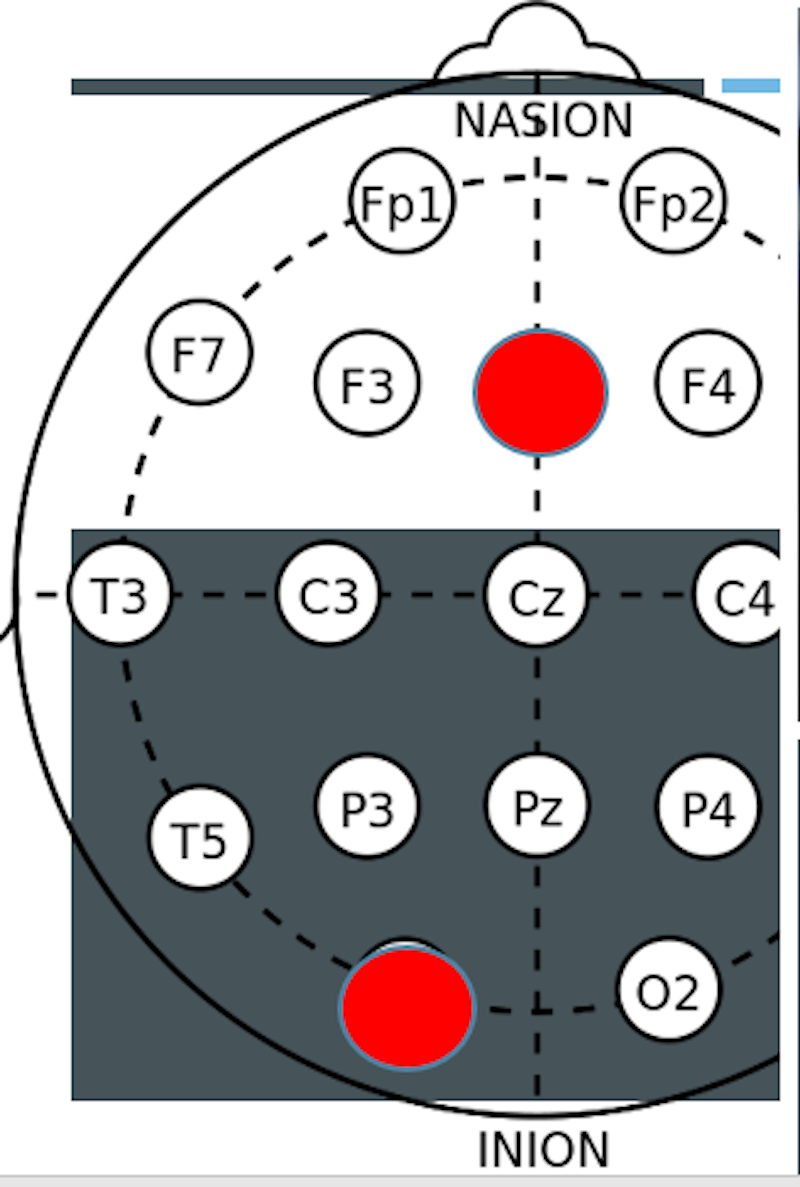
We offer the 5 site ClinicalQ as our primary assessment as the majority of Swingle Clinic clients do not need a 19 Channel Normative Brain Map. For most, the extra time and expense is not necessary to target the symptoms or goals for which they are seeking our assistance. In sum, 19 channel full capping and analysis is expensive overkill for information that is usually not required for the vast majority of conditions (symptoms) we treat. We often feel monies would be better spent on actual treatment rather than the collection of superfluous information. For a select few however, 19 site mapping is not only recommended, but necessary.
Who Should Get a 19 Channel Normative Brain Map?
For anyone seeking treatment for stroke, significant closed / traumatic head injury, as well as a known or suspected seizure disorder a Normative (19 Channel) brain map can be central to / for efficacious treatment. 19 Channel maps give us information on coherence, phase lag and provide a closer look at amplitude asymmetry. (In plain English this means the maps show us about connectivity; areas of the brain that due to damage cease talking to each other or in contrast talk to each other too much. It also shows us areas or systems that are much more or less powerful than they should be for efficient brain function –Hence your symptoms). Some forms of normative mapping also provide information on deeper structure and brain circuitry.
The Grey Areas on Grey Matter:
Complex learning disorders associated with any form of apraxia or dyspraxia, chromosomal or genetic disorders, developmental delay and speech delay can also benefit from normative mapping. Elderly clients fearing dementia or Alzheimer’s can potentially benefit from 19 Channel Brain Maps as well. Delusions, illusions / hallucinations, suspected or diagnosed Schizophrenia can also benefit from further insight provided from full capping. In these cases, we start with a Clinical Brain Map and somewhere between 3 and 10 sessions your Neurotherapist may discuss the potential benefits of a Normative Brain Map and, further determine where in the treatment cycle said Normative Brain Map might be of assistance to the advancement of treatment.
Children and adults on the Autistic spectrum sometimes also benefit from information provided by a 19 Channel Normative Brain Map. Although some of these clients would benefit from a Normative Brain Map on intake, many are not able to sit still enough, are fearful of the process, or have sensory issues that inhibit the wearing of the 19 point electrode cap. For these clients we carefully assess timing versus quality of data collection. With such clients spontaneous and / or situational change may also occur (e.g., a child is having a very good day and the time is ripe for data collection), and parents / guardians should be prepared for such. Conversely, a 19 channel map may be booked and thereafter changed to single site (channel), sequential point or 5 point (5 channel) mapping to ensure that the data collection process is both efficient and the information obtained is useful for treatment planning (e.g., not corrupt due to high impedance / poor signal(s), and / or high artifact AKA false readings due to excessive movement or expressed discomfort).
A good rule to follow:
Yet another grey area is concussion. If you are seeking treatment due to symptoms attributed to a concussion, a 19 Channel Normative Brain Map is the recommended route. If you are not directly symptomatic but have had three sequential concussions, again, the information from a 19 Channel Normative Map could be helpful in guiding your treatment. Many individuals are not symptomatic, and the brain has successfully repaired itself. Others do not believe they are symptomatic but, once in treatment, the brain reveals patterns that suggest that a 19 Channel Brain Map would be helpful. Again, if your BCIA Certified Neurotherapist sees such patterns, they will discuss the potential benefits of seeking Normative, as opposed to, or in addition to, Clinical comparatives to aid with the precision of your treatment / training.
When a 19 Channel Mapping is a choice:
Curiosity: If you are curious and have the luxury of funds to afford a 19 Channel Normative Map, it can be an interesting experience of self-discovery but it is surely not necessary.
Known Risk: If you know you are at risk of head injury and would like a reserve road map back to brain health. E.g., elite athletes with a couple of ‘minor’ head injuries in sports known for major head injury such as boxing, MMA, various forms of racing (ski & car), football / rugby, bobsledding, etc., will often chose to have Normative mapping.
Reserve: Families of wealth will sometimes also choose to have themselves or their children mapped ‘just in case’. Much like some choose to preserve umbilical cord blood ‘just in case’.
More on BRAIN DRIVING & PHOTOSONICS
Brain Driving first released as Braindryving TM was another brain child (pun intended 😉 ) of Dr Paul Swingle. Brain Driving involves the pairing of precise frequencies of sound and light and feeding them (back) to the brain to influence its efficiency. It is classic / passive conditioning (as opposed to operant / active conditioning).
‘Feeding’ the brain through frequency is nothing new. Light and sound have long been used to influence the human state. Think strobe lights in discos to excite dancers, slow glows to calm in spas, and meditate in living rooms. Sound influence has also arguably been used for centuries if not millennia. Think deep drumbeats to induce trance / meditative states or conversely incite or convey fear, all rhythm or frequency dependent.
Photosonics: Using independent or complementary light (photo) and to a much lesser extent sound (sonic) was common in early Neurotherapy practice. What was new, was Dr Paul Swingle’s direct pairing of photosonic components directly with brain activity itself! –Specifically, pairing and unpairing light and sound with the real-time-EEG to directly (rather than indirectly) influence brainwave production.
Brain Driving can be an extremely efficient form of Neurotherapy when applied discriminately. At Swingle Clinic we find it particularly helpful for conditions wherein volition can be affected (e.g., stroke and head injury), challenged (e.g., Autism), or contraindicated in training (as with some pernicious forms of ADHD and anxiety-based disorders) wherein ‘willing’ the brain to quiet is counter-productive.